Listing summary
NAP8 Local Resources
The challenges we face in reaching a wide range of patients are common to the ones many of you experience when engaging with patients locally. Perhaps you were trying to audit or redesign services, or prepare or revise patient information. Some of the responses to these challenges are also common.
PatientsVoices@RCoA is a group of volunteers who help the College improve the delivery of safe, more effective, patient-centred care to enhance patients’ experience of anaesthesia and perioperative care. It’s vital for us to understand and represent the views of diverse communities, as we live in one of the most multicultural countries in the world.
The LLP team has been busy delivering a range of webinars and workshops as part of our commitment to helping and supporting doctors on their individual and collective training paths. One important webinar was a pre-ARCP preparation workshop held in January 2025, with trainers and trainees contributing useful guidance, information and top-tips to navigate the process. This supplemented previous introductory guidance covering reviewing the curriculum and creating ESSRs, HALOs and SLEs.
Many of these professionals receive some formal training in perioperative care during their careers, but many do not. Many anaesthetists recognise that optimal perioperative care is crucial in reducing the number of people waiting for surgery, improving outcomes when they do have surgery, and optimising long-term health.
To do this, we need a skilled multiprofessional workforce with consistent training and education. NHS England therefore contracted the Centre for Perioperative Care (CPOC) to develop a multiprofessional medical curriculum in perioperative care. CPOC – a cross-specialty collaboration which works with patients and partner organisations to promote and develop perioperative care – is ideally placed to harness the expertise of professionals and patients, reflecting both users and providers of perioperative care.
Looking through the Health Education England (HEE) Gold Guide, you can find the information about an Out-of-Programme Career Break (OOPC). OOPCs allow trainees an opportunity to step away from training to give them time to pursue other interests, including interests not connected with medicine. This is different from the other out-of-programme options which are more related to clinical training (OOPT), clinical experience (OPPE) or research (OOPR). This led me down a path I will never regret.
It’s beneficial for all anaesthetists to manage cognitive load at work, but also for anaesthetists to implement these principles when teaching in theatre.
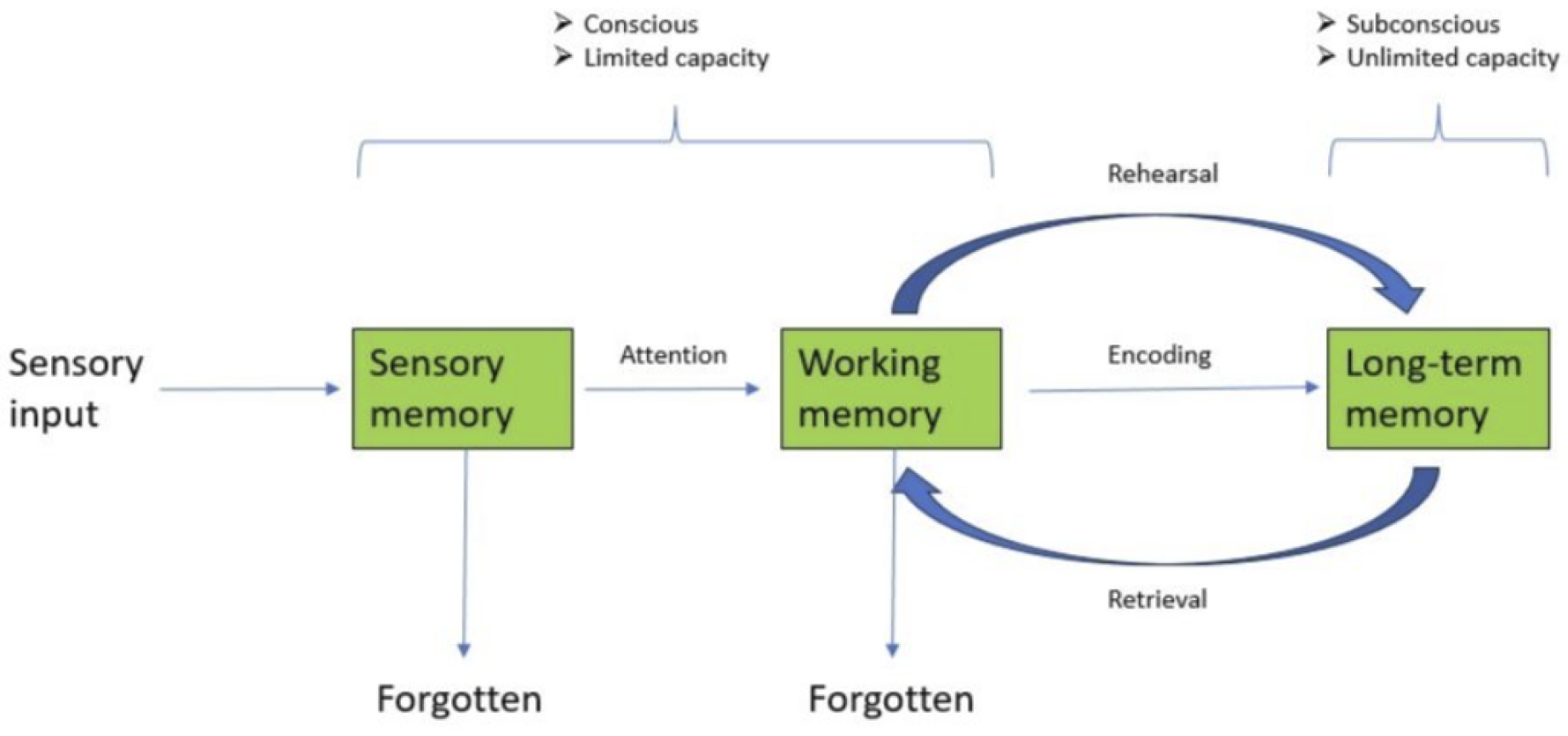
Cognitive load theory has been developed from the Modal model of memory described by Atkinson and Shiffrin. This details how information is received, encoded, stored and retrieved during learning (see An illustration of the Modal model of memory by Dr Thomas Walters). Incoming information is consciously held and processed within working memory, before being encoded into long-term memory. Working memory has a limited capacity, and information within it is transient and forgettable. Once encoded into long-term memory, information is organised in schema, with a seemingly unlimited capacity. Working memory can hold five to nine pieces of information at a time. However, if required to process this information, capacity is significantly reduced.
As with any practical procedure, there are many ways to learn, but it is practically impossible to become competent or excellent at regional anaesthesia without regular hands-on patient experience. Recent UK-wide surveys revealed a large proportion of Stage 3 trainees unable to perform all Plan A blocks independently, and found that only a small proportion of consultants and specialists felt confident teaching all these blocks to trainees. It has also been seen that the higher the number of blocks trainees perform, the more confident they feel. Currently, ‘getting numbers’ and achieving the required competence, feels challenging.
We acknowledge that there is an inevitable period of adjustment following curriculum transition, but many of our trainee colleagues still feel their current skills in this area are inadequate for their level of training. To prevent this becoming a perpetual challenge this issue must be proactively addressed across all stages of training.
{kind=link}